
| Virtual Environments to Support People Living with HIV |
||
Ethics• The participants’ consent to participate in the experiments was informed and uncoerced. • Each participant had the right to refuse to participate in the research or to withdraw at any stage. • Support mechanism was in place to protect the participants against any foreseeable physical, psychological or social harm which might be experienced during the experimental process. • Personal information pertaining to the participants was kept confidential.
1. Forest scene depicting the campfire in the VE
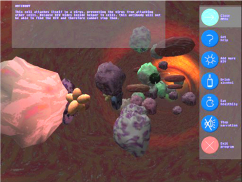
2. Screenshot of Bloodstream VE
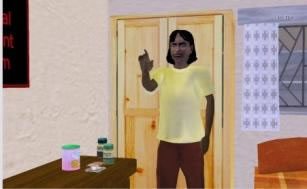
3. Sandi Introduces Hygiene in the Kitchen
|
We have been investigating the use of Virtual Environments (VEs) to support people living with HIV and Aids since 2001. Novel Information Technology solutions can assist us in dealing with the HIV/AIDS pandemic with the provision of information and social support. We have developed three prototype applications using an adapted user centred design method to provide emotional and informational support to people living with HIV. Our prototype virtual environments (VEs) provided narratives of responses to HIV diagnoses, factual information related to the virus within the human blood stream, and nutritional and hygiene information. Our approach is to build systems and then to reflect on the experience of using such a system: this is the normal approach of experimental computer science. We adopted the view that VEs could provide social support to HIV+ people. We developed our research over three studies which are presented below: Prototype 1: Virtual Support Group (Emotional Support) We developed a low cost desktop PC based system using custom software. The system implements a VR walkthrough experience of a tranquil campfire in a forest (Figure 1). The scene contains four interactive avatars who relate narratives compiled from counselling sessions with HIV/Aids patients. These narratives cover three aspects of HIV infection: receiving an HIV+ diagnosis, intervention, and coping and living with an HIV+ status. Prototype 2: Simulation of the HI-Virus (Informational Support) This study visualized the human circulatory system by modelling a blood vessel and the action of the HI-virus in the bloodstream (Figure 2). The progression of the virus can be divided into three distinct stages: 1) Infection; 2) Virus Progression; 3) Advanced Virus Progression — referred to as “Full Blown Aids”. In this project, stages 1 and 2 were modelled and interactively showed the effects of the virus on an infected person’s immune system. Recommendations of good behaviours and activities (such as exercise and eating well) were given within the environment, and the effects of these were interactively experienced by the user Prototype 3: HIV House (Social and Informational Support) to HIV+ Pregnant Women The aim of this VE was to incorporate the experiences gained in the previous prototypes and allow for new material; we therefore chose an expandable design. We also wanted an environment that users would find familiar. We created a council house in which each of the rooms could be made to serve a different function and contain information and interactions corresponding to the activities that are associated with that room. Thus the narratives of Study 1 were presented in the lounge, the action of HIV, from the second study, on the (interactive) television in the bedroom, and the other rooms allowed other forms of support and counselling. The third study included an extensive knowledge of nutrition and hygiene (Figure 3), presented in the kitchen. Other possible extensions to this environment would be the provision of educational content on sex issues (presented in the bedroom), issues relating to mother-to-child transmission (MTCT) in a baby room and information relating to antiretroviral therapy in the bathroom. Participants All had very little, if any, previous computer experience. The following groups, all from the intended target groups in deprived communities, tried out the prototype systems:
Perceived Quality “The people in the house – they taught me a lot. Um … and then the lounge, talking about their problems and … So the people inside the house were great. Um ja, ja, but I’ve learnt a lot from the, from Sindi [Sandi, the virtual character in the kitchen] and the kitchen. I’ve learnt a lot from her because … er, that’s where that I’m not quite clued up when it comes to nutrition.” Empowerment from very use of technology “…they [other HIV positive individuals] can also learn things from the computer, learning you can do more things even if you are HIV positive....I think that the computer is also there for people to know that “I’m still living, I can do what the other people who haven’t got HIV do, I can do it, like this computer thing.” “Yoooh it was very …. First it was a great opportunity because it’s my first time (using a computer) and it is interesting. I wish I can do more, so that I can learn more … so interesting.” |
|


Co-Researcher
Dave Nunez
Clinical Psychologist
Mignon Coetzee
Students
Sabeeha Hamza: first prototype
Amber Kisch, Warren Prior, Eric Savage: 2nd prototype
Sarah Brown: final system
Virtual Identity is not a real identity
- One major benefit here is virtual people are open about their status
- Participants remain anonymous